India is home to over 77 million people living with diabetes — the second-highest number in the world. Of these, nearly one in three will develop some form of diabetic eye disease, known as diabetic retinopathy, in their lifetime. What makes this condition particularly dangerous is that it causes no pain and no visible symptoms in the early stages, yet can lead to permanent, irreversible blindness if left untreated.
At Dr. Agarwal’s Eye Hospital, our retina specialists answer the same five questions from diabetic patients every day. Here are those questions — and the answers every diabetic needs to know.
1. What is Diabetic Retinopathy?
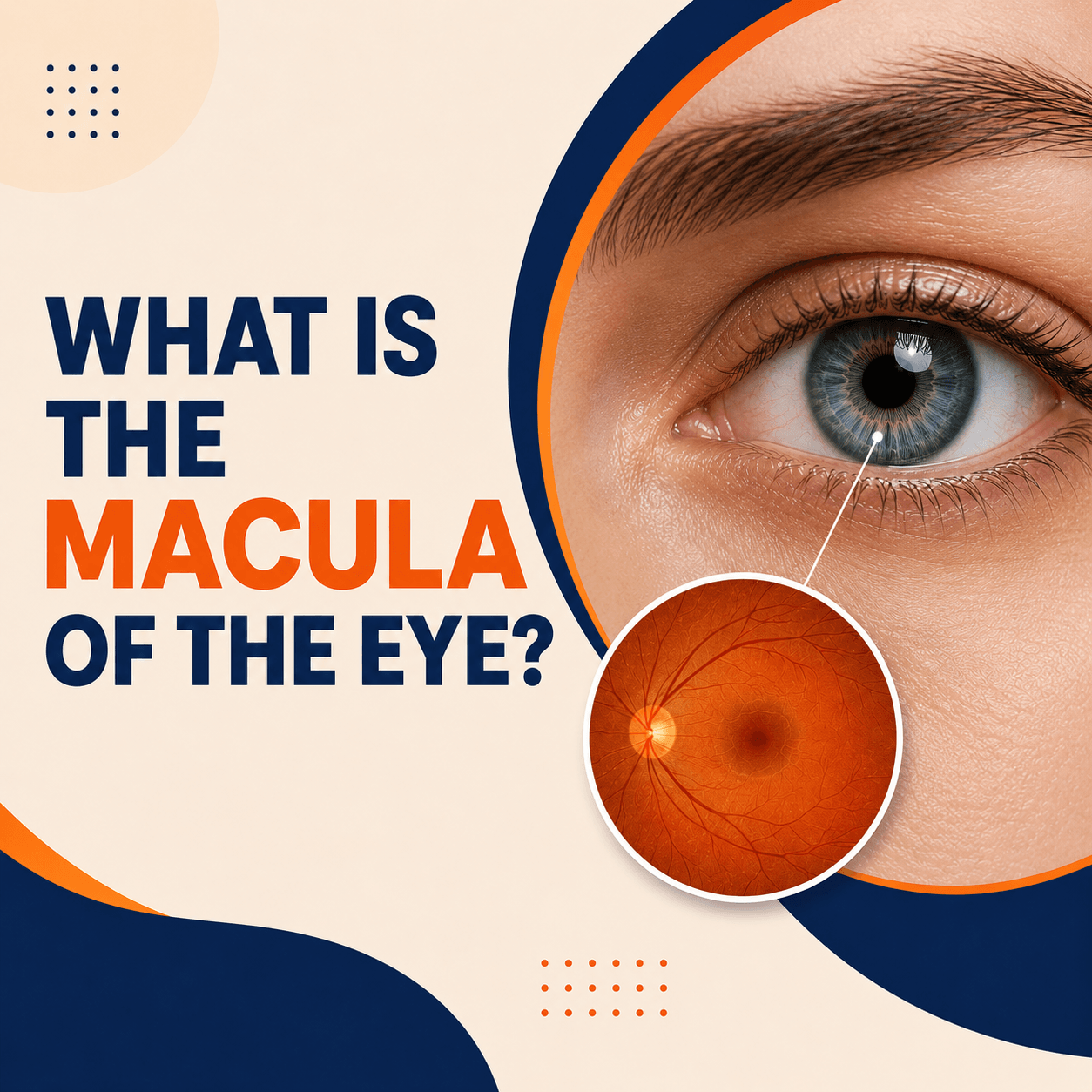
Diabetic Retinopathy is a blood vessel related disorder seen in diabetic patients affecting retinal blood circulation. The retina is the photo sensitive layer at the back of the eye.
Long standing high blood sugar levels cause thickening of small blood vessels supplying blood to the retina. This results in bleeding within the retina and swelling in some cases.
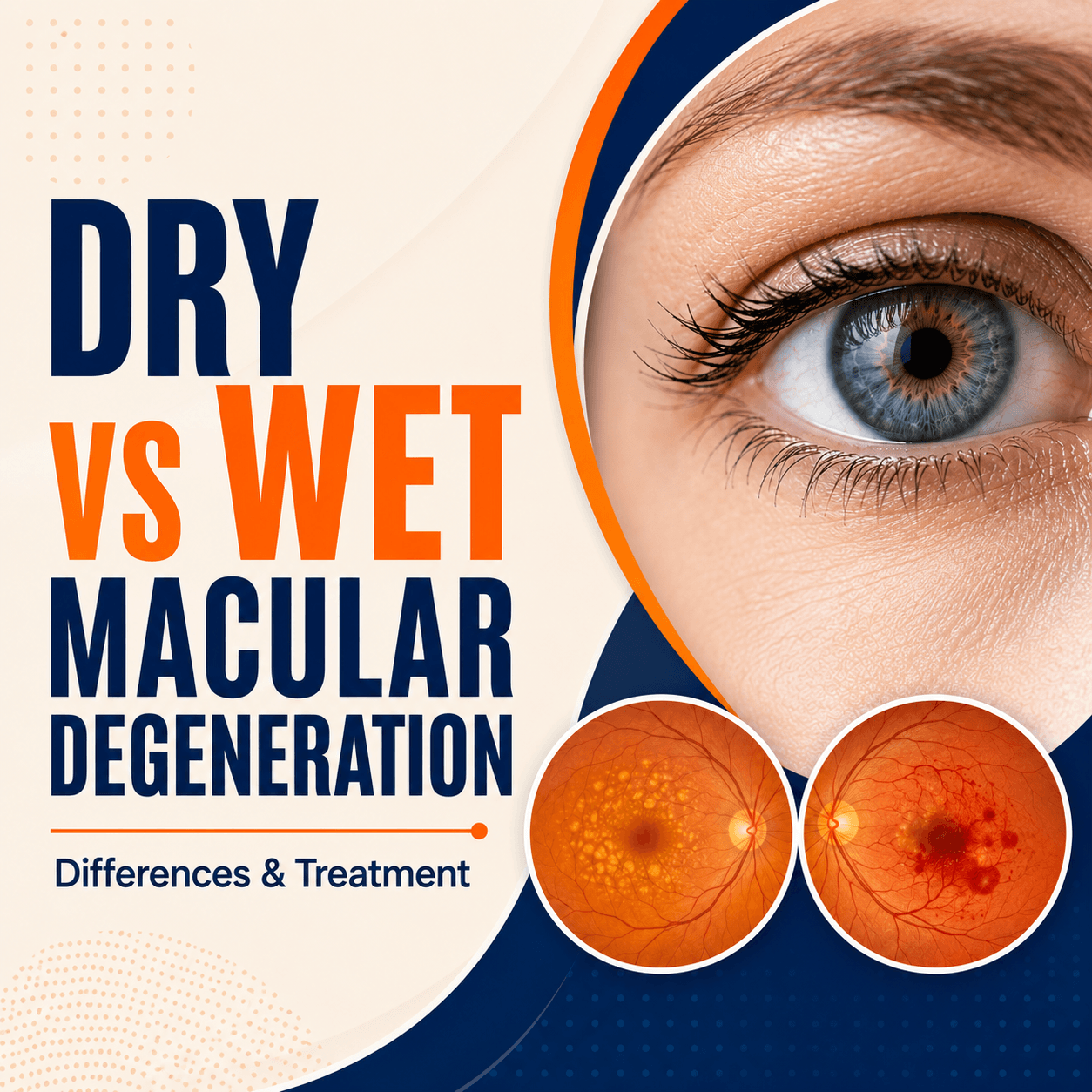
These stages may be associated with swelling in the central part of retinal called as macular edema. Macular edema is a major cause of blindness in diabetic patients.
Diabetic Retinopathy is a complication of long-standing Diabetes Mellitus — it is not a standalone eye disease, but a consequence of poorly controlled blood sugar over time.
Diabetic retinopathy progresses through two main stages:
- Non-Proliferative Diabetic Retinopathy (NPDR): The early stage, characterised by microaneurysms (tiny bulges in blood vessels), small haemorrhages, and hard exudates. Vision may still be normal at this stage.
- Proliferative Diabetic Retinopathy (PDR): The advanced stage, where abnormal new blood vessels grow on the retina and into the vitreous. These fragile vessels bleed easily and can cause severe, sudden vision loss.
Both eyes are usually affected, though one eye may be worse than the other.
2. Do All Diabetics Develop Diabetic Retinopathy?
The answer is no, not every diabetic will develop this condition. However, several risk factors significantly increase the chances of developing this blinding condition. These associated risk factors are: uncontrolled blood sugar (HbA1c above 7%), hypertension, kidney disease, high cholesterol levels, obesity, smoking and pregnancy.
One of my patients recently came to me with a decrease in vision in his left eye. On a thorough check-up he was found to have Proliferative Diabetic Retinopathy in both eyes the most advanced stage of the disease. On evaluation, his blood sugar levels were very high, as were his cholesterol levels.
That is why I say the eye is a window to many diseases. A fundus examination can reveal early signs of systemic conditions, including diabetes mellitus, hypertension, high cholesterol, myasthenia gravis, multiple sclerosis, and many brain tumours.
If you have been diagnosed with diabetes, do not wait for symptoms. By the time vision problems appear, significant damage may already have occurred. Early detection through a routine fundus examination can prevent blindness.
3. Who Is at Higher Risk of Developing Diabetic Retinopathy?
Patients with Type 1 diabetes are at higher risk than those with Type 2. The risk of developing diabetic retinopathy is almost 90% after 15 years of having Type 1 Diabetes Mellitus. For Diabetic Retinopathy, the duration of diabetes is a stronger risk factor than blood sugar control alone. However, maintaining good blood sugar control (HbA1c below 7%) significantly slows progression.
If diabetes is associated with hypertension, kidney disease (nephropathy), high cholesterol, or pregnancy, retinopathy progresses faster and requires more frequent monitoring.
Screening Recommendation for High-Risk Groups:
- Type 1 Diabetics: Begin annual retinal screening within 5 years of diagnosis.
- Type 2 Diabetics: Begin annual retinal screening at the time of diabetes diagnosis.
- Diabetics with Hypertension: Every 6 months, or as advised by your specialist.
- Diabetics with Kidney Disease: Every 6 months — nephropathy and retinopathy often progress together.
- Pregnant Diabetics: Each trimester and at 6 weeks post-delivery.
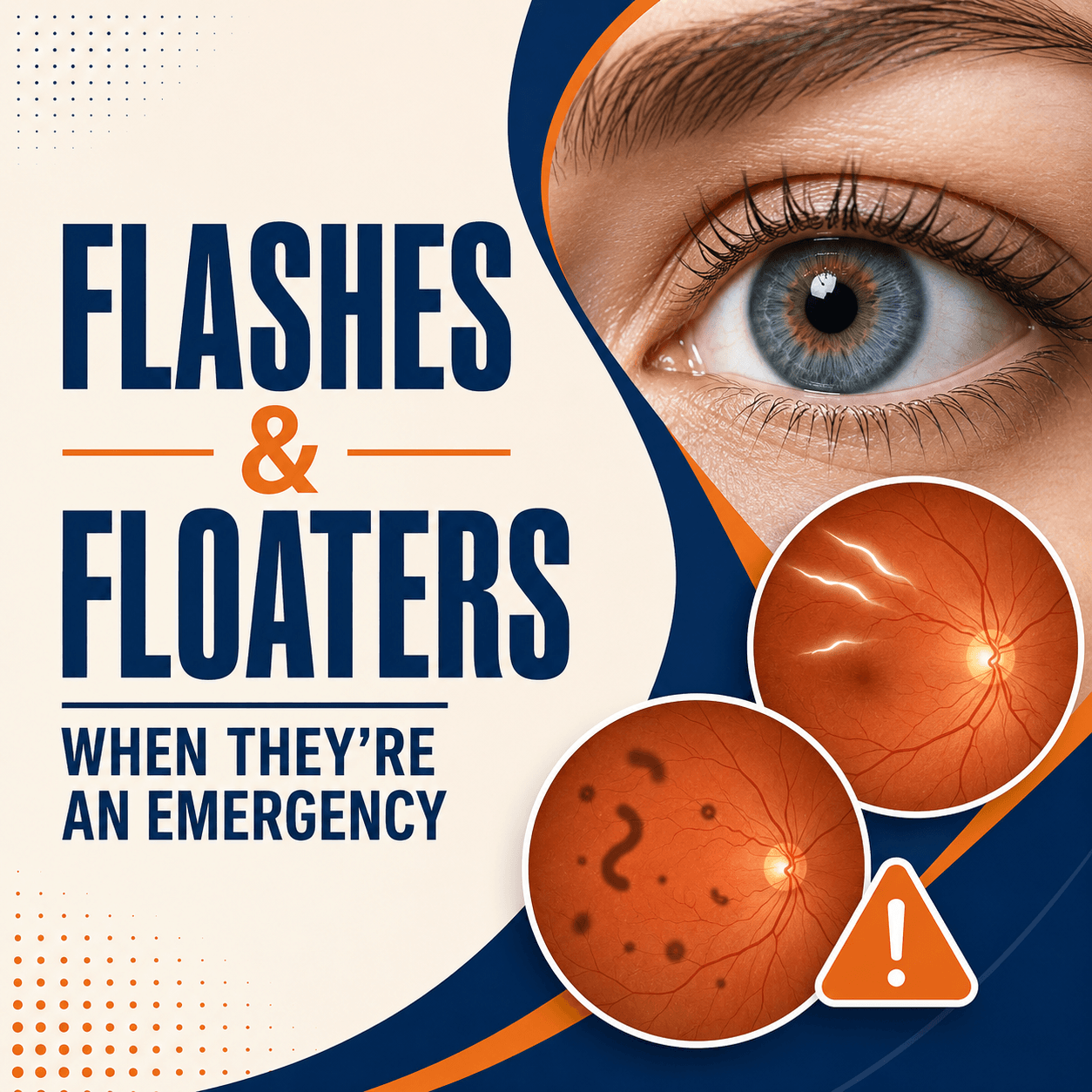
4. How Will I Know I Have Diabetic Retinopathy?
The most important thing to understand about diabetic retinopathy is that in the early stages, it is completely silent there are no symptoms, no pain, and no vision changes that the patient would notice.
Symptoms such as blurred vision, diminution of vision, distortion of vision, and the appearance of floaters or dark spots occur only in the later and more advanced stages of the disease. By this point, substantial and often irreversible damage has already occurred.
The only reliable way to detect diabetic retinopathy early is a dilated fundus examination, a painless retinal check-up performed by an eye specialist after dilating your pupils.
During this examination, the specialist uses an ophthalmoscope or a slit lamp with a special lens to directly view the retina, optic nerve, and blood vessels. In some cases, fundus photography or Optical Coherence Tomography (OCT) may also be performed to get a more detailed image.
If you are diabetic and have not had a retinal examination in the past 12 months, book one today, even if your vision feels completely normal.
5. What Can Be Done to Treat Diabetic Retinopathy?
The best way to tackle this condition is to detect it at the earliest stage and begin treatment, preventing progression to late stages that are irreparable
This can be done by scheduling a comprehensive dilated retina check-up, ideally annually, from the day you are diagnosed with diabetes.
Treatment options for diabetic retinopathy depend on the stage of the disease:
- Medical Management (All Stages)
- Control blood sugar: Keeping HbA1c below 7% is the single most effective way to slow retinopathy progression.
- Control blood pressure: Target below 130/80 mmHg.
- Control cholesterol: Statins may be prescribed if cholesterol is elevated.
- Laser Photocoagulation (Moderate to Severe NPDR / Early PDR)
A laser is used to seal leaking blood vessels or destroy abnormal new vessels. This is performed as an outpatient procedure and is painless under topical anaesthesia. It is highly effective at preventing further vision loss but does not restore vision already lost.
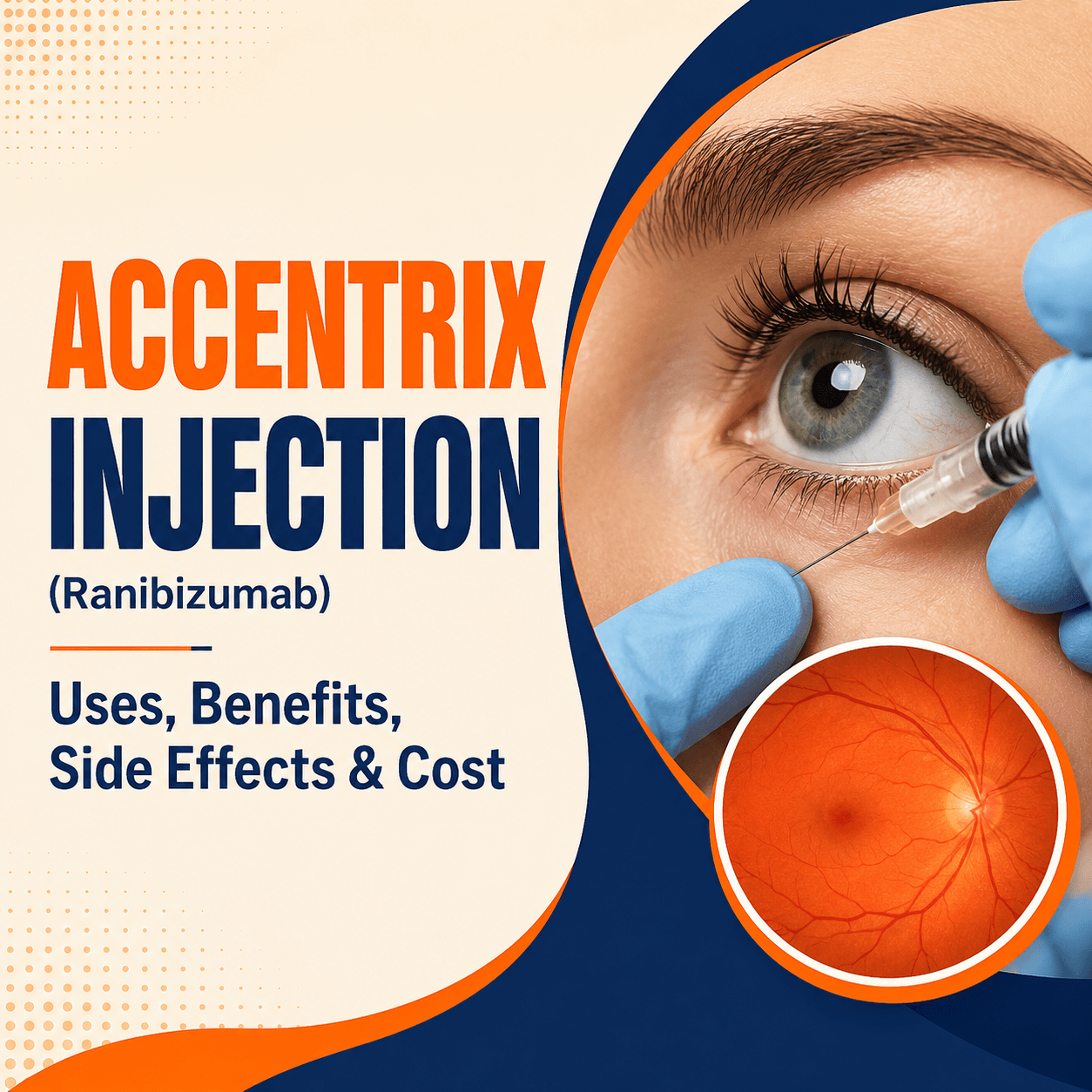
- Anti-VEGF Injections (Macular Edema / PDR)
Medications such as Ranibizumab, Bevacizumab, or Aflibercept are injected directly into the eye (intravitreal injection) to reduce swelling and stop the growth of abnormal blood vessels. Multiple sessions may be required. These injections are the current gold standard treatment for diabetic macular edema.
- Vitrectomy (Advanced PDR with Vitreous Haemorrhage or Tractional Retinal Detachment)
In advanced cases where the vitreous (jelly inside the eye) has bled or the retina has detached, a surgical procedure called vitrectomy is performed. The surgeon removes the blood-filled vitreous and repairs the retina. This is a major surgical intervention performed under local or general anaesthesia.